928
Views & Citations10
Likes & Shares
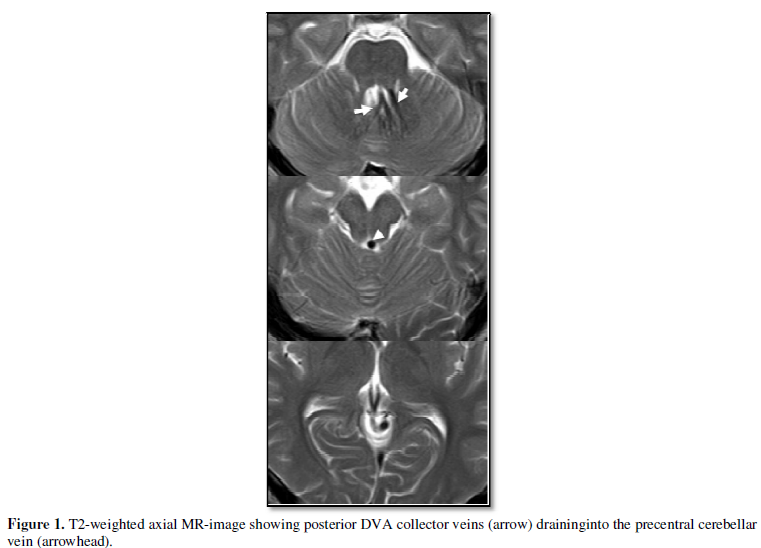
A 15-year-old boy presented to our hospital
with headache after head trauma caused by a traffic accident. T2-weighted axial
MR-images demonstrated the deep medullary veins of the cerebellum converging on
the roof of the fourth ventricle. These veins drained into the subependymal
vein, which then drained into the precentral cerebellar vein (Figure 1).
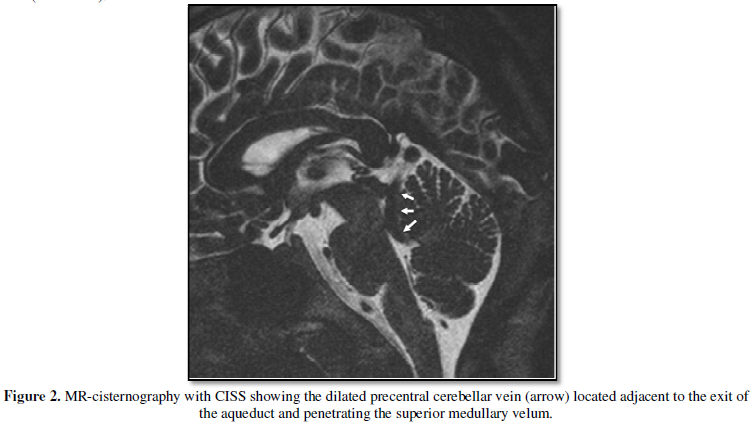
MR-cisternography with 3D Fourier transformation constructive interference in
steady state (CISS), which can depict the venous anatomy when
is surrounded by CSF, demonstrated a dilated precentral cerebellar vein located
in the fourth ventricle. This dilated precentral cerebellar veinran adjacent to
exit area of the aqueduct of Sylvius, penetrated the superior medullary velum
and finally drained into the vein of Galen (Figure 2). The lesion was diagnosed
as a developmental venous anomaly (DVA). MR-images did not show any hemorrhage
or ventricular dilatation. This young man did not require any specific medical
treatment for his venous anomaly.
Developmental venous anomalies (DVAs) are
known as congenital intracranial vascular lesion. Most DVAs are asymptomatic;
however, they may occasionally cause obstructive hydrocephalus and should be
considered in cases of chronic or intermittent headaches (2,3). Paulson et al
reported a case with hydrocephalus caused by the DVA passing through the
orifice of the aqueduct and referred 10 previously reported cases which had presented
with hydrocephalus (2). Their conclusion was that no surgical treatment was
necessary for the DVAs for itself, but CSF diversion might be necessary in some
cases. Although MR-images demonstrated a dilated precentral cerebellar vein
adjacent to the aqueduct in our case which presented with headache, an aqueduct
stenosis resulting in hydrocephalus was not present and surgical intervention
was not considered necessary.
1.
Lee
C, Pennington MA, Kenney CM. MR evaluation of developmental venous anomalies:
medullary venous anatomy of venous angiomas. AJNR 1996;17:61–70.
2.
Paulson
D, Hwang SW, Whitehead WE, Curry DJ, Luerssen TG, Jea A: Aqueductal developmentalvenousanomaly as an
unusual cause of congenital hydrocephalus: a case report and review of the
literature. J Med Case Rep. 2012 Jan 11;6:7.
3.
Giannetti
AV, Rodrigues RB, Trivelato FP. Venous lesions as a cause of sylvianaqueductal
obstruction: case report. Neurosurgery. 2008;62:E1167–1168. discussion E1168
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Pathology and Toxicology Research
- BioMed Research Journal (ISSN:2578-8892)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)


